Neck and Shoulder pain is an extremely common complaint, and there are many
common causes of this problem. It is important to make an accurate
diagnosis of the cause of your symptoms so that appropriate treatment
can be directed at the cause. If you have Neck and shoulder pain, some common
causes include:
- Abnormalities in the bone or joints
- Trauma
- Poor posture
- Degenerative diseases
- Tumors
- Muscle strain
- Poor posture
The shoulder is a ball and socket joint with a large range of
movement. Such a mobile joint tends to be more susceptible to injury.
Shoulder pain can stem from one or more of the following causes:
- Strains from overexertion
- Tendonitis from overuse
- Shoulder joint instability
- Dislocation
- Collar or upper arm bone fractures
- Frozen shoulder
- Pinched nerves (also called radiculopathy)
Due to continuous pain in an over strained muscle there are tendency to develop myofascial trigger point because of which there will be continuous dull and nagging pain in the muscle.
Trigger points, also known as trigger sites or muscle knots, are hyperirritable spots in skeletal muscle that are associated with palpable nodules in taut bands of muscle fibers.
The trigger point model states that unexplained pain frequently
radiates from these points of local tenderness to broader areas,
sometimes distant from the trigger point itself.
Compression of a trigger point may elicit local tenderness and or referred pain.
Pictures shown below are the common sites of myofascial trigger point pain :-

pain.

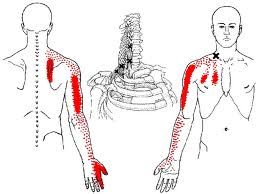
Pain radiating down throughout the arms and fingers.
Trigger Point therapy can reduce pain, increase movement, and allows the muscles to
lengthen and become stronger again. To treat Trigger Points, heavy pressure must
be applied to the Trigger Point. Light pressure is not effective for treating Trigger
Points, and in fact may increase spasms as the muscle tries to protect itself, leading
to increased and more constant pain. In contrast, moderate to heavy pressure
applied to a Trigger Point causes the pain to initially increase, but then as the
muscle relaxes the pain will fade.
Points, and in fact may increase spasms as the muscle tries to protect itself, leading
to increased and more constant pain. In contrast, moderate to heavy pressure
applied to a Trigger Point causes the pain to initially increase, but then as the
muscle relaxes the pain will fade.
Pressure should be applied slowly and released slowly for best results. The pressure






should be maintained until there is a change in pain. If there is no decrease in pain
after one minute, stop the pressure—this is probably not a Trigger Point! After
applying pressure to Trigger Points, the relaxed muscle should be stretched. If the
muscles are not returned to normal length, there is a greater likelihood the Trigger
Points will reoccur. Stretching is safer and less painful after the Trigger Points have
been treated.
after one minute, stop the pressure—this is probably not a Trigger Point! After
applying pressure to Trigger Points, the relaxed muscle should be stretched. If the
muscles are not returned to normal length, there is a greater likelihood the Trigger
Points will reoccur. Stretching is safer and less painful after the Trigger Points have
been treated.
Few self trigger point release techniques:-
Please consult your Physiotherapist before applying these techniques.
Physical Therapy:
Physical therapy is an important aspect of treatment of almost all
orthopedic conditions. Physical therapists use different modalities to
increase strength, regain mobility, and help return patients to their
pre-injury level of activity.


















